
After a long Christmas break I'm back to teaching and what a better way to start the year with some blood gas interpretation.
The first thing to think about before doing the gas is "will a venous sample suffice?". This is often over looked due to habit or requests from a old school consultant. The H+, Bicarbonate and Lactate are accepted to be the same between arterial and venous samples and the correlation with pCO2 for hypercarbia is regularly debated. The pO2 is obviously not present in venous samples and the sample should be compared with the patients current oxygen saturation. A good summary article of these issues can be found
here.
There are 5 key questions to ask when interpreting an ABG.
1. What is the oxygenation like? Is there
respiratory failure?
Type 1 - pO2 <8 pCO2<6
Type 2 - pO2 <8 pCO2 >6
 2
2. Look at the
H+, is there
acidosis (H+ >45) or
alkalosis (H+<45)?
3. Look at the
CO2, is it raised (
respiratory acidosis) or lowered (
respiratory alkalosis)? Does this fit?
4. Look at the
Bicarb, is it raised (
metabolic alkalosis) or lowered (
metabolic acidosis)? Does this fit?
5. Is there any
compensation? Either
Full, Partial or None
Remember there only 4 broad answers to blood gas interpretation and you should know a handful of causes for each.
 Respiratory Acidosis
Respiratory Acidosis - These people have a high CO2 and are hypoventilating. Using a top down approach the causes are:
Respiratory centre - Drugs i.e. opoids
Peripheral nerves - Guillain-Barré syndrome
Neuromuscular junction - Myaesthenia gravis
Chest Wall - Obesity, severe kyphoscoliosis
Airways - COPD, Severe asthma
Respiratory Alkalosis - These people are the opposite and are hyperventilating. People hyperventilate commonly due to anxiety and pain, however, more serious conditions such as P.E. and Subarachnoid Haemorrhage need to be remembered
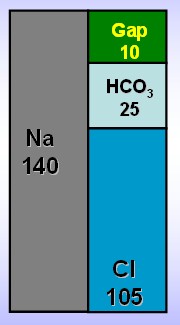
Metabolic Acidosis - These people have extra acid or have lost base. You can calculate their anion gap to see if there are extra acids by :
(Na+ +
K+) - (Cl- -
HCO3-).
The normal range is 12 - 18.
(The reason it is not 0 is due to the weak acid affects of albumin and lactate)

If it is raised then it is due to one of the following:
MUDPILES.
Methanol intoxication
Uremia
Diabetic or alcoholic ketoacidosis
Propolyene Glycol
Isoniazid
Lactic acid
Ethylene glycol intoxication
Salicylate intoxication
If the gap is normal then it is likely due to
Renal tubular acidosis, Diarrhea or Gastrointestinal fistula
Metabolic Alkalosis - This is more likely from the loss of acid rather than gaining base as even with infusing bicarbonate the pH barely moves. Acid is lost through
vomiting or through the kidney with
diuretics or
Conn's syndrome.
It is possible to have a mix of two i.e. respiratory and metabolic acidosis by combining two diagnosis' from above. I appreciate that some people out there may prefer using the strong ion difference rather than the traditional Henderson Hasselbalch approach outlined above. For undergraduates the traditional method is more than adequate and exams will feature this approach. For those keen for a deeper understanding see Scott Weingarts brilliant acid base series
here,
Here are 5 examples and I want you to work them through using the 5 questions and tell me the acid base disturbance and a possible cause.
|
|
|
1
|
2
|
3
|
4
|
5
|
|
H+
|
(35-45)
|
62
|
29
|
27
|
84
|
103
|
|
pCO2
|
(4.6- 6)
|
10.3
|
2.7
|
5.8
|
2.5
|
7.8
|
|
pO2
|
(10.5 - 13)
|
6.5
|
18.1
|
11.4
|
16.3
|
8.8
|
|
Bic
|
(22-26)
|
32
|
25
|
35
|
9
|
6
|
Scroll down for the answers.
1.Type 2 Respiratory Failure with a partialy compensated respiratory acidosis COPD. 2. Uncompensated Respiratory Alkalosis Anxiety attack. 3. Uncompensated compensated metabolic alkalosis Vomiting. 4. Partially compensated metabolic acidosis DKA. 5. Mixed respiratory and metabolic acidosis Obese Sepsis














{kind=link}